

Background:
Hereditary thrombocythemia (HT) has been reported in Japanese and African populations in association with S505N, and N35K c-Mpl mutations, respectively. A novel Pro106Leu germ-line mutation in the c-Mpl gene has recently been shown to be associated with HT in Arabic population. Clinical and bone marrow (BM) features of Pro106Leu mutation are largely unknown.
Methods:
The molecular genetic databases at two tertiary hospitals in Riyadh, King Abdulaziz medical city (KAMC) and King Saud University medical city (KSUMC), were searched to identify all patients (pts) with MPL Pro106Leu mutation. Clinical and pathological data were retrospectively collected. BM aspiration and biopsy were independently reviewed retrospectively by two consultant hematopathologists and agreement was reached by a consensus review.
Simple descriptive statistics were used to summarize the results. A univariate subgroup analysis, comparing the hematologic parameters between the homozygous and heterozygous genotypes was conducted using Pearson Chi-Square and t-tests.
Results:
A total of 115 pts with Pro106Leu MPL mutation were included, 86 (75%) from KAMC and 29 (25%) from KSUMC. All pts were ethnically Arabs. Median age was 33 years (yrs) (range: 0.4-68), 65 (56.5%) were female, and 31 (27%) were pediatric pts (age <18 yrs).
MPL Pro106Leu mutation was homozygous in 87 (75.7%) pts, and heterozygous in 28 (24.3%).
Spleen was enlarged in 3 (3%) pts, not documented in 15 (13%), and normal in 97 (84%). History of bleeding was documented among 11 (10%) pts. Thrombosis history was positive in 5 (4%) pts only, unavailable in 6 (5%), and negative in 104 (90%). Family history of thrombocytosis was reported in 46 (40%), but family history was not documented in 20 (17%).
Common comorbidities include: autoimmune disease in 33 (29%), diabetes 21 (18%), and hypertension 20 (17%). Reasons for MPL testing was: abnormal routine blood work 79 (69%), family history of thrombocytosis 23 (20%), or others 13 (11%).
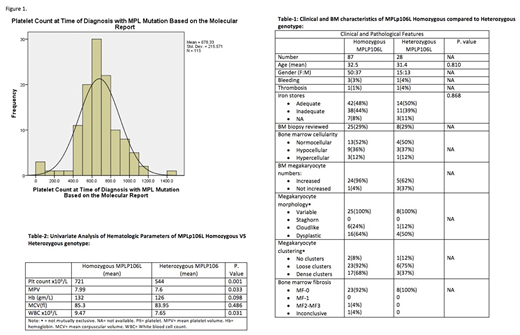
Thrombocytosis [platelet (plt) counts > 450 x109/L] was documented in 107 (93%) pts, normal in 4 (3.5%), and low in 4 (3.5%) at the time of diagnosis of Pro106Leu mutation. See figure 1. The median plt count at the time of diagnosis of MPL Pro106Leu mutation was 667 x 109/L (range: 13-1473). The median mean plt volume was 8 fL (range 6.1-10.2), white blood cell count 8.4 x 109/L (2.46-68.35), absolute neutrophil count 5 x 109/L (1.01- 21.19), hemoglobin 132 gm/L (85-148), mean corpuscular volume 84.1 fL (57-117.3), mean corpuscular hemoglobin 27.7 pg (18-37.5), mean corpuscular hemoglobin concentration 327 g/dL (300-351), and red cell distribution width 13.6 (10.9-22.8). Ferritin less than 30 was seen in 40 (35%) pts, 27 of whom were women. No ferritin done in 14 pts. Iron stores (based on bone marrow, ferritin and iron saturation) were adequate in 56 (49%), inadequate in 49 (43%), and not documented in 10 (9%).
BCR-ABL, JAK2 and CALR were only detected in 1 pt each. One pt was not tested for CALR mutation. All other pts were negative for the three mutations.
Out of all 115 pts, 33 (29%) had an evaluable BM. BM cellularity ranged from 20-100 %, 12/33 (36%) were hypocellular, 17/33 (52%) normocellular, and 4/33 (12%) hypercellular. Megakaryocyte (meg) morphology revealed dysplastic changes in 20 (60%) (hypolobated megs or with separated lobes), only 7 (21%) of cases had cloudlike megs but none had staghorn or giant megs as described in essential thrombocythemia. BM megs were increased in 29 (87%). Small size megs were seen in 15/33 (45%). Clustering of megs was seen in the majority of the cases 30/33 (90%) of whom, 29(87%) had loose and 20 (60%) dense clusters.
On univariate analysis (see tables 1-2), homozygous genotype was associated with higher plt count.
Total of 65 (57%) pts were prescribed aspirin, and 16 (14%) hydroxyurea. At the time of last follow-up 114 (99%) of pts were alive. The median follow-up was 7.8 yrs from the time of thrombocytosis (ranged from 0-24.8). No case developed disease progression to myelofibrosis. One pt was diagnosed with T-lymphoblastic lymphoma and later died from treatment complications and another pt was diagnosed with CML.
Conclusion:
Pro106Leu mutation is associated with marked thrombocytosis at a younger age with a low risk of thrombosis. Homozygous genotype is associated with a significantly higher plt count. BM usually shows either normo- or hypocellular marrow with increased megs proliferation, and clustering.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal